

SEROLOGY TESTING & IMMUNITY
SEROLOGY TESTING & IMMUNITY
COVID-19 IN NEW ZEALAND

Introduction
Serology provides us with interesting insights into immune responses to Covid-19 infection and vaccination, however we must ensure that our interpretation of data is tempered by close consideration of the limitations of serology.
Serology testing for SARS-CoV-2 is finally available in New Zealand (as of 28/11/22). The public can now book an appointment at Rako Science, where a PictArray Elisa serology kit will be used to determine the presence or absence of anti-spike antibodies (anti-S) and anti-nucleocapsid antibodies (anti-NC). Anti-S may be present following either vaccination or infection, Anti-NC may be present following infection (but not vaccination).
Detection of these antibodies is used to predict vaccine efficacy via a process called immunobridging: where the presence of antibodies is assumed to be reflective of immune status. Immunobridging cannot provide definitive answers on immune status because immune responses extend far beyond just antibody production. Antibody detection provides, at best, an approximation for immunity. In the April 2022 FDA VRBPAC meeting, Dr Peter Marks discusses immunobridging:
“There is not a clear, perfect, immune correlate of protection, and so we’re using poor man’s immune correlates of protection here.”
The FDA has granted EUAs based off immunobridging endpoints for the following groups:
Pfizer - 6 months to 4 year olds
Pfizer - 5 to 11 year olds
Pfizer - 12 to 15 year olds
Pfizer - booster #1
Pfizer - booster #2
Moderna - 6 months to 17 year olds
Moderna - booster #1
Moderna - booster #2
Serology testing is used in studies to identify the prevalence or incidence of past infections via the detection of anti-NC. This methodology has a large error rate and will underestimate the number of covid-19 infections in the vaccinated portion of the population. PictArray are carrying out one such study in New Zealand over the next six months.
The PictArray study will be examining immune responses in the vaccinated only. It will not cover natural immunity alone. Around 15% of New Zealanders remain unvaccinated, and by now a significant proportion of these will have been exposed to SARS-CoV-2.
Vaccinated and unvaccinated individuals respond differently to SARS-CoV-2. The unvaccinated who recover from infection are more likely to develop broad and lasting immunity. Vaccination, after a brief period of protection, appears to impair the development of broad and lasting immunity, and this phenomenon may be implicated in the plethora of rapid repeat infections, and the lack of herd immunity that we are currently seeing.
What does serology tell us?
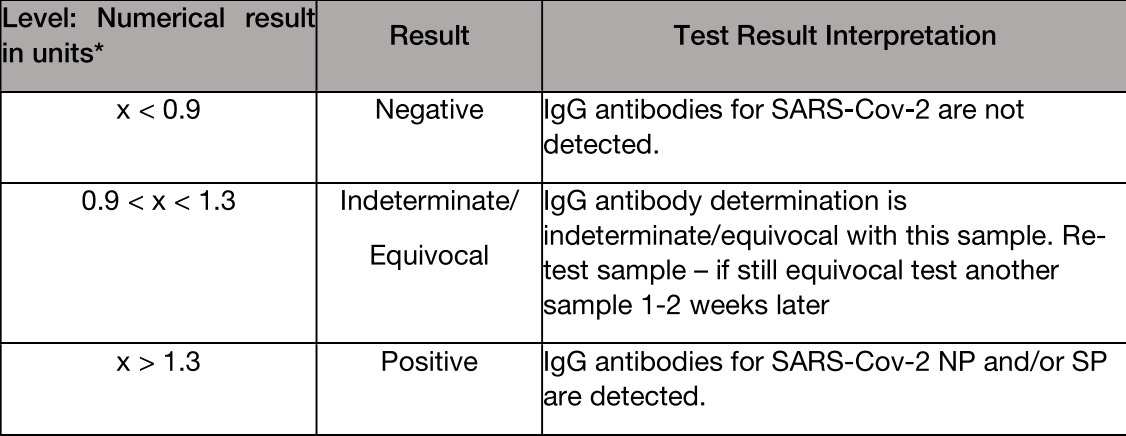
The PictArray test detects the presence of two antibodies - one against the spike protein (anti-S antibodies) and the other against the nucleocapsid (anti-NC antibodies) - and reports them qualitatively using a ratio:
I was the third member of the New Zealand public to get the test. I am unvaccinated and had a mildly symptomatic covid infection about 140 days (just under 5 months) prior. Rako are not collecting data on infection or vaccination history, but I discussed mine with the technician. He predicted that I would be a 4 (positive) for spike, and negative for nucleocapsid. I predicted that I would be positive for nucleocapsid, and low or negative for spike.
The immune responses reflected in serology differ depending on infection history and vaccination status. A vaccinated individual is more likely to be positive for anti-S (in higher levels following vaccination compared to infection), and less likely to be positive for anti-NC (following an infection).
I was hoping that my prediction would be correct. Not because I am certain of what the implications are, but because the available evidence has led me to suspect that higher anti-NC:anti-S may be a more optimal ratio (based upon an assumption that higher levels of antibody are preceded by higher levels of antigen*). Nucleocapsid antibody is associated with a more durable immune response which persists across SARS-CoV-2 mutations. High spike protein is associated with the development of long covid. Decent studies are needed to pin down the details, however, and serology only offers one piece of the immune puzzle.
Serology does not definitively tell us if we are immune to covid, though it may offer some insight. The extent to which the presence of spike and nucleocapsid antibodies predicts protection against covid infection and disease is uncertain, as immunity is not limited to antibody production.
Serology can confirm a past infection in people who generated an anti-NC response. Not all past infections will be picked up however, because:
Not everyone produces anti-NC following an infection: Vaccinated people are less likely than unvaccinated people to produce anti-NC.
Anti-NC is not produced immediately after an infection: If serology is done too early, it may fail to pick it up.
Anti-NC wanes over time: If serology is done too late, it may fail to pick it up.
Anti-NC is sometimes used in studies as an estimate of population disease prevalence or incidence, however this method will underestimate disease burden, especially in the vaccinated. Using serology to measure vaccine efficacy against infection will result in a falsely inflated vaccine efficacy.
Serology can detect if anti-S has been produced. Anti-S may be present following infection and/or vaccination. The likelihood of detection is also subject to timing of serology testing relative to infection and vaccination. Anti-S levels tend to be higher in vaccinated individuals.
The interpretation below is offered with the test. It is an oversimplification, for example on line 2: A negative NP (anti-NC) and a positive SP (anti-S) could also indicate previous infection in which the production of anti-NC was blocked following vaccination.

Immunity through vaccination
Spike, but not nucleocapsid
Vaccination induces the production of spike antibodies, but not nucleocapsid antibodies.
A SARS-CoV-2 virus particle is made up of a collection of proteins and genetic material. Viral proteins that can be recognised by our immune system are called antigens. Nucleocapsid protein (NC) and spike protein (S) are two such antigens. The spike protein facilitates the entry of the virus into our cells. Our immune system sees antigens as the enemy, and mounts a defence campaign (which includes antibodies and T cells) against them.
The mRNA vaccines train the body to produce spike protein endogenously. The immune system forms memory B cells (which generate antibodies) and T cells specific to this spike protein. The hope is that, when the SARS-CoV-2 virus enters our body, we have a ready made army of highly specific immune cells which will recognise the spike protein, prevent viral particles from entering our cells, and kill any cells that do get infected.
Unfortunately, the vaccine has not worked exactly as hoped. Vaccination is associated with a period of decreased risk (although this is likely, at least partially, an artefact of inappropriate vaccination categorisation), but predominantly an increased risk of infection (depending on time since injection, number of injections, and infection history). Whilst spike protein may provide initial protection via antibody production, it is inherently damaging to cells (1), which may contribute to:
Severe illness from covid
Adverse events following vaccination
Negative efficacy for infection.
Increased risk of covid infection (negative efficacy) in the vaccinated
Risk of infection increases for the first 1-2 weeks following receipt of mRNA vaccines, then decreases for a few months (some of this decrease can be explained by misclassification of vaccine status), and then increases again.
A December 2022 preprint study (2) attempted to quantify the protective effects of the bivalent booster against infection from the strains represented in the booster in a group of 51,011 employees at the Cleveland Clinic. They calculated a VE (vaccine effectiveness) of 30% for the booster relative to prior vaccinations.
The VE may be somewhat illusory, however, because infections were not counted in individuals who received the bivalent booster until a week has passed. In February 2021 researchers (3) from the NIH and Public Health England examined data from the Israeli vaccination programme and found that the incidence of covid infections more than doubled within the first week following vaccination, and did not drop below pre-vaccination levels for over two weeks. This means that the Cleveland Clinic infections caused by the bivalent booster in that first week were counted in the dose 3 group - having the effect of making the bivalent booster appear relatively effective.
The bivalent booster study (2) also found that:
“Risk of COVID-19 increased with time since the most recent prior COVID-19 episode and with the number of vaccine doses previously received…The higher the number of vaccines previously received, the higher the risk of contracting COVID-19”

The graph above is cumulative on a per-population basis. The graph below, showing the infections in New Zealand for the last six months, is daily/weekly snapshots on a per-population basis. Our New Zealand data is largely consistent with the results of the Cleveland Clinic study.

The authors published further research (4) from the Cleveland Clinic in the journal, Clinical Infectious Disease, and found that:
“Among those previously infected, receipt of 2 compared with 1 dose of vaccine was associated with higher risk of COVID-19.”
Immune Imprinting (aka Original Antigenic Sin)
As the SARS-CoV-2 virus mutates, the nucleocapsid protein is highly conserved (5) (it remains recognisable to our immune system), but the spike protein is not (it becomes progressively more unrecognisable). The original mRNA vaccines produce spike that is equivalent to the Wuhan strain of Covid-19. The newer bivalent vaccines produce an omicron strain, however the virus has since mutated away from the strain in these vaccines.
Because the mRNA vaccines were formulated to address the original Wuhan spike protein, there has been some concern that immune imprinting may occur. This happens when the immune system is trained to respond to a specific antigen (in this case the Wuhan spike protein). As the virus mutates, and that original specific antigen becomes less common as it is crowded out by new proteins, the immune system continues to focus its response on the original antigen, thus failing to mount a comprehensive immune response against the current dominant antigens. This would render vaccinated individuals less able to mount immune responses to these subsequent variants, leaving them more vulnerable.
A paper (6) published in the journal Cell (March 2022) analysed human lymph nodes to investigate whether antibodies stimulated by mRNA vaccination differ from those generated by infection. The authors found evidence of immune-imprinting:
“Viral variant infection elicits variant-specific antibodies, but prior mRNA vaccination imprints serological responses toward Wuhan-Hu-1 rather than variant antigens.”
The graph below shows that the immune response of vaccinated individuals is disproportionately trained on the Wuhan strain of the virus.


Immunity through infection (natural immunity)
Some people argue that natural immunity through infection should be avoided at all cost, because the risks from covid infection are too great. This school of thought relies on restrictions and vaccination to protect people from ever becoming infected. There are obvious and insurmountable holes in this argument:
Neither vaccinations nor restrictions prevent infection. Covid-19 is highly contagious. Virtually everyone will be exposed repeatedly for the foreseeable future. Following a brief period of protection, vaccination appears to drive infection rates up (possibly through spike-mediated immune changes, and the suppression of nucleocapsid production).
It has been known since early 2020 that the risk from covid infection is highly stratified. By far the greatest burden falls on the elderly and immune-suppressed. The majority of the population is not at risk of a severe covid outcome, and thus restrictions are neither a proportionate nor sustainable response.
The NC protein (which is produced only in response to infection, but not vaccination) is highly conserved across SARS-CoV-2 variants (5) - meaning that it remains recognisable to our immune memory even as the virus mutates. Thus, the presence of infection-induced anti-NC antibodies implies a more durable immune response against covid. There is an abundance of literature showing that natural immunity is more robust and lasting than vaccine-induced immunity.
Natural immunity through infection is superior to immunity through vaccination
There are an abundance of papers demonstrating that immunity from natural infection is stronger and more durable, so it is unclear as to why media and state messaging claim that natural immunity is inferior.
A paper in the journal Clinical Infectious Diseases (2022) (7) described the “largest real-world observational study” comparing natural immunity (via previous SARS-CoV-2 infection) to vaccine-induced immunity (Pfizer). The study examined over half a million people and found that vaccinated, Covid-19 naive individuals had a 13 times higher odds ratio of breakthrough infection, and a 27 times higher odds ratio of symptomatic disease compared to previously-infected but unvaccinated people. The authors noted that:
“Waning of protection against infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) conferred by 2 doses of the BNT162b2 vaccine begins shortly after inoculation and becomes substantial within 4 months.”
“Naturally acquired immunity confers stronger protection against infection and symptomatic disease caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 2-dose vaccine-induced immunity.”
“Our study matches the CDC report, examining cohorts in California and New York, demonstrating that infection-induced protection was more substantial than vaccine induced immunity during the Delta period.”
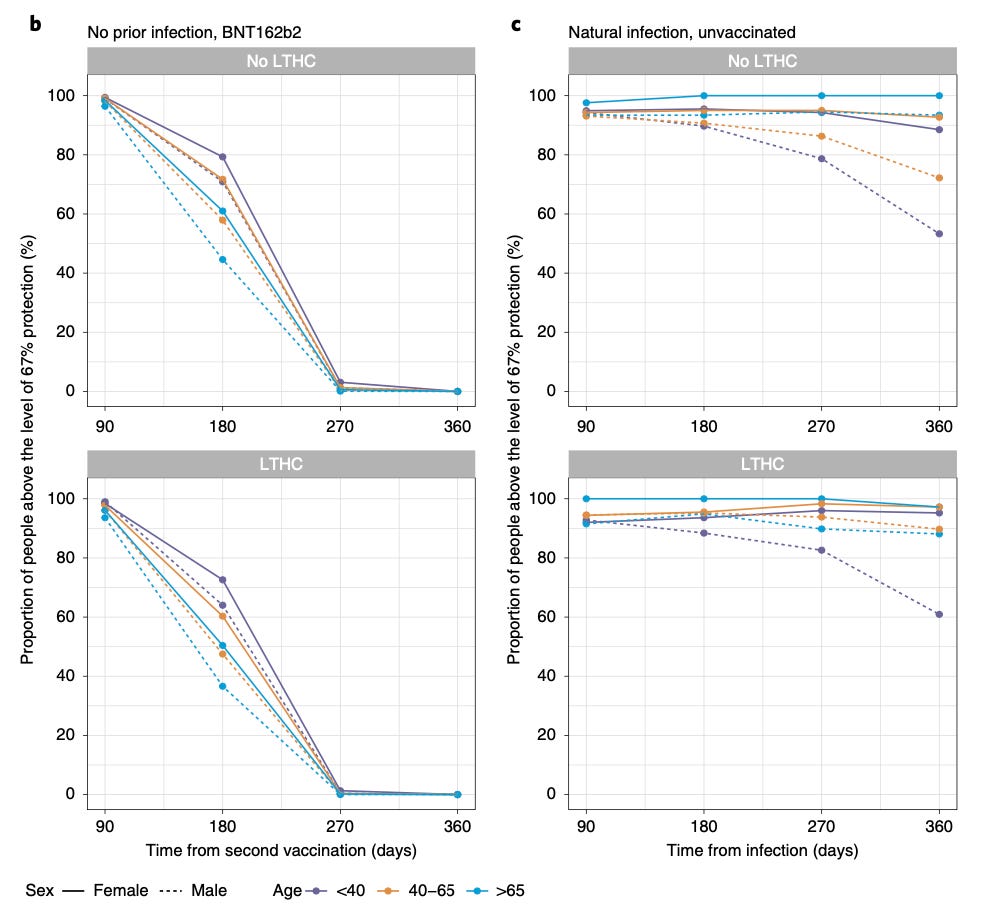
A team from Oxford University published a study (8) in the journal Nature Medicine which used correlates of protection alongside antibody responses to predict protection against covid. They found:
“At least 67% protection against infection was estimated to last… for 5–8 months after two BNT162b2 doses in those without prior infection and for 1–2 years for those unvaccinated after natural infection”
The charts below show that the proportion of people (with and without long term health conditions) who remain at least 67% ‘protected’ for at least a year is significantly higher in the unvaccinated, natural infection group (c) compared to the uninfected, vaccinated (Pfizer) group (b):
A study (9) reported in the New England Journal of Medicine (September 2022) investigated the protection from vaccination (Pfizer) versus natural immunity against infection and hospitalisation in children aged 5-11 years. Unvaccinated children with natural immunity had generally longer lasting protection against reinfection compared to children with ‘hybrid’ immunity (vaccination and prior infection).
Graphs E and F from the study show the effectiveness of vaccination (E) and natural immunity (F) against hospitalisation over time. At first glance (the top two graphs), it appears that there are high and persistent levels of protection from both, however on closer inspection we can see that the X axes are not equivalent: ‘Weeks’ is used for the vaccinated, and ‘Months’ for the unvaccinated. I added a vertical red line to graphs E and F (the bottom two graphs) to show the 5 month mark for both the vaccinated and unvaccinated. I then added a horizontal red line to show what level of protection each group had at the 5 month mark. The vaccinated are at c77% protection at 5 months, and the slope of the line indicates that this is dropping away. The unvaccinated are at c98% protection at 5 months. Ten months into the study the unvaccinated are still in the high 80s. This is a significant difference in immunity.
The authors must have been aware that, without closer inspection, this graphic was misleading.

Hybrid Immunity
Hybrid immunity has become something of a buzz word in the news. As it became obvious that protection from the vaccine alone was not what we had originally expected, it became widely reported that hybrid immunity - from a combination of both infection and vaccination - was superior to both vaccine-induced immunity and natural immunity.
The New England Journal of Medicine published a paper (10) in June, 2022 offered this rather convoluted conclusion:
“Among persons who had been previously infected with SARS-CoV-2 (regardless of whether they had received any dose of vaccine or whether they had received one dose before or after infection), protection against reinfection decreased as the time increased since the last immunity-conferring event; however, this protection was higher than that conferred after the same time had elapsed since receipt of a second dose of vaccine among previously uninfected persons. A single dose of vaccine after infection reinforced protection against reinfection.”
The suggestion was that hybrid immunity is superior, and the results were widely shared. The graphic below shows:
Unvaccinated individuals (red) with natural immunity from a prior infection.
Vaccinated individuals (green/grey) who have never had an infection.
Vaccinated individuals (blue/purple) who have had an infection (hybrid).
A shorter bar indicates a better result - it means a lower infection rate in the group (the X axis is the infection rate as time passes).
At first glance, the Hybrid group is smashing it:
Group B (vaccinated, but not infected) are shown to have very high infection rates, indicating relatively poor immunity.
Group C (hybrid immunity) have the shortest bars, and thus appear to have the best immunity.
Group A (unvaccinated with natural immunity) are somewhere in the middle.
On closer inspection however, this is not what the graphic reveals, because the study authors made the rather odd decision not to use comparable time frames on their Y axes.
I have pasted another copy of the graphic below, and removed the lower three red unvaccinated bars (8-12+ months) because there are no comparable figures for these amongst the vaccinated. I then drew a vertical blue line down from the ‘unvaccinated 6-8 months’ group in order to directly compare them with the ‘hybrid 6-8 months’ group.
It is now apparent that the unvaccinated did better than the hybrid immunity group, and were the most protected overall.
The authors must surely have been aware that, without close inspection, this graphic was misleading.

Mis-categorisation of vaccination status
The superiority of the unvaccinated infection rate above is probably underestimated due to the widely accepted practice of considering study participants as unvaccinated until 1-2 weeks after their injection. Because the first two weeks following a vaccination are a period of increased risk of infection, a significant number of infections in the vaccinated are lumped into the unvaccinated data, as demonstrated in the graphic below. The graphic also explains why at least some of the vaccine efficacy in each subsequent booster is illusory.


Mis-categorisation of vaccination status also affects hospitalisation and death data in the following manner:
Example: An individual receives dose one of the Covid-19 vaccination:
If they become a covid case before seven days have passed – they are classified as an unvaccinated covid case.
If they become a covid hospitalisation before seven days have passed – they are classified as an unvaccinated covid hospitalisation.
If they die from or with covid before seven days have passed - they are classified as an unvaccinated covid death.
If the individual becomes a covid case six days after they are vaccinated, get hospitalised two weeks later, and dies a week after that - four weeks after they were vaccinated - they are classified as an unvaccinated case, an unvaccinated hospitalisation and an unvaccinated death. Thus, if someone dies with or from covid four weeks after they were vaccinated - the death can be added to the unvaccinated tally.
Miscategorisation of vaccination status is omnipresent in government data sets. It also infects published scientific literature. For example, a Danish paper (21) published in the journal Nature in September 2022 found that the risk of household transmission of SARS-CoV-2 was increased in the unvaccinated and decreased in the boosted, relative to those who are fully vaccinated. The chart from the paper below shows us that compared to the fully vaccinated, a primary case was 37% more likely to be infectious if they were unvaccinated, and 20% less likely to be infectious if they were boosted. In addition to the usual vaccination misclassification described above, the authors included anyone who had been vaccinated with a single dose in the unvaccinated group; and rather astonishingly, they included unvaccinated individuals with previous infection in the fully vaccinated group. As explained in this article, previously infected but unvaccinated individuals generally have more robust immunity. These misclassifications will likely make the unvaccinated appear to do worse than they are, and the vaccinated appear to do better. The Danish study is investigating the effect of vaccination, however given that it does not provide data based on true vaccination status, the reported results are rendered meaningless.

Spike
Our immune system produces anti-S antibodies in response to spike protein - presented either through vaccination or infection. There has been some suggestion that the spike protein may not have been the right antigen to target for vaccination purposes because:
Spike protein is not highly conserved across mutations, and therefore is less likely to induce lasting immunity.
Spike protein causes harm to cells, (1) so most vaccinated individuals will be exposed to a double whammy of spike through both infection and vaccination.
Vaccination induces higher levels of spike production than infection
Vaccinated individuals produce higher levels of anti-S antibodies compared to the unvaccinated, and sustain them for a long time:

Busch et al (2021) (11)
What are the implications of having high levels of spike circulating in our bodies?
“The biodistribution, quantity, and persistence of vaccine mRNA and spike antigen after vaccination and viral antigens after SARS-CoV-2 infection are incompletely understood but are likely to be major determinants of immune responses.” (6)
We know that spike can cause harm, but there is uncertainty around how the amount and longevity of spike corresponds to the level of harm. Unfortunately, there was very little research conducted into the biodistribution of mRNA vaccines prior to their rollout. Pfizer submitted a pre-clinical animal model biodistribution study (12) to the Japanese health regulator in May 2020, the results of which ought to have provided the impetus for immediate and comprehensive human studies - but this did not eventuate.
As an example of a finding that warrants further investigation, the Pfizer paper used 48 hours as the cut off point for evaluating the concentration of lipid nanoparticle (the ‘packaging’ in which the mRNA vaccines are distributed around the body) in the ovaries of mice, however lipid nanoparticle was still rising at the 48 hour point, so we have no way of knowing what happens to the concentration past this point (though we can see that it likely kept rising):

A paper (6) published in the journal Cell (March 2022) found that the germinal centres within lymph nodes of vaccinated individuals produced significant amounts of spike protein for an extended period of time (the study took samples up to 60 days following dose 2). Unvaccinated people produced smaller amounts of spike protein.
“Immunohistochemical staining for spike antigen in mRNA-vaccinated patient LNs varied between individuals but showed abundant spike protein in GCs 16 days post-second dose, with spike antigen still present as late as 60 days post-second dose.”
They also found significant levels of spike in the plasma of vaccinated individuals. They did not continue to monitor these levels beyond a week.
“At least some portion of spike antigen generated after administration of BNT162b2 becomes distributed into the blood. We detected spike antigen in 96% of vaccinees in plasma collected 1–2 days after the prime injection, with antigen levels reaching as high as 174 pg/mL…the concentrations of spike antigen in blood quickly decrease although spike is still detectable in plasma in 63% of vaccinees 1 week after the first dose.”
Given that the spike protein can cause cell damage, the amount of spike produced in response to both infection and vaccination is important. No doubt there is significant individual variation, which may partially explain why some individuals get very sick from covid-19, and some get very sick following vaccination.
Spike and Long Covid
A team from Harvard Medical School published a paper (1) in the journal Clinical Infectious Diseases which measured antigen levels (spike and nucleocapsid proteins) in the blood of a small group of covid patients and PASC (‘long covid’) patients. Elevated levels of spike, but not nucleocapsid, were present in most of the PASC patients. The recovered covid patients did not have elevated levels of spike. The authors hypothesised that:
“The detection of spike in PASC patients months after diagnosis suggest the presence of replicating viral reservoirs.”
The authors explained how circulating spike protein could give rise to PASC symptoms:
“spike contains structural motifs that skew the T-cell receptor repertoire, possibly accounting for the hyperinflammatory response observed in severe COVID-19 and multisystem inflammatory syndrome in children... spike alone has been shown to induce dysfunction in pericytes, vascular endothelial cells, and the blood–brain barrier”
But the authors admitted a flaw in their theory, which they were unable to explain: If there are indeed persistent viral reservoirs in the bodies of PASC patients, why was nucleocapsid not also detected? The lack of nucleocapsid suggests that there is no viral reservoir, in which case, where does the spike come from? Is it feasible that persistently high spike may instead be due to a residual reservoir of non-immune cells transfected with vaccine mRNA and churning out spike protein, inappropriately and unregulated since their activity is not regulated by the normal cytokine system?
The authors ruled out vaccination as a reason for the high spike based on a study (13) which examined vaccinated individuals with no history of infection, and found low circulating spike (anti-S antibody was high, but spike protein was low). But these two studies were not examining the same populations - one group had been infected, one had not. Is there something unique about spike production in someone who has been both infected and vaccinated? We know that the vaccinated produce more anti-S antibodies - so is it possible that they can produce more spike compared to unvaccinated individuals?
The key point here is that there is still much that is unknown about the production and kinetics of the spike protein following vaccination.
Nucleocapsid
Vaccination impairs the production of anti-NC antibodies in subsequent infections
In August 2021 a paper (14) in the Journal of Infection examined the production of anti-NC antibodies following SARS-CoV-2 infection in vaccinated (Pfizer) versus unvaccinated healthcare workers. Only 26% of the breakthrough infections in the vaccinated led to the production of anti-NC antibodies, compared to 82% of unvaccinated infections.
In October 2021 the UK Health Security Agency released their Week 43 report (15). On page 25 of the report there was a brief note suggesting that vaccination impaired the production of anti-NC antibody in subsequent infection:
“(jii) recent observations from UK Health Security Agency (UKHSA) surveillance data that N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.”
The above statement was subsequent to a preprint (16) from Public Health England which found:
“a statistically significant reduction in geometric mean N antibody level following both single dose and full vaccination for both Alpha and Delta infections.”
The authors established that unvaccinated individuals produced anti-NC antibodies readily, and maintained them over a long period. 91% of unvaccinated individuals were still seropositive at 9 or more months post-infection.
“We conclude that N-antibody levels are lower following vaccination and differ by variant.”
In July 2022 an NIH study (17) investigated the usefulness of estimating past infection status by using anti-NC detection in vaccinated versus unvaccinated participants of the Moderna trial. They found that anti-NC antibodies were produced in 40% of vaccinated individuals upon subsequent infection, and in 93% of infected but unvaccinated individuals. The authors concluded that vaccination status ought to be considered when interpreting seroprevalence data based on anti-NC antibody testing.
The following month a longitudinal serological surveillance study (18) also found that vaccination impairs anti-NC antibody production.
“Another notable finding from our study was that breakthrough infections often did not generate a robust anti-nucleocapsid antibody response, which, to our knowledge, has not been reported previously.”
The figure below shows that unvaccinated individuals (on the left) generated significant anti-NC antibodies which persisted for months. Vaccinated individuals (on the right) produced only 54% of the anti-NC produced by the unvaccinated.
The authors warn that:
“evaluating the prevalence of infection via anti-nucleocapsid serology may significantly underestimate the true prevalence of breakthrough infections in previously vaccinated populations.”

Nucleocapsid antibodies persist for a long time
A paper (19) published in the journal Scientific Reports (July 2022) examined the persistence of anti-NC antibodies in unvaccinated individuals with prior infection and found that they remained at significant levels for at least 15 months, and likely longer.

The implications are substantial
If vaccination impairs the production of nucleocapsid, then vaccination might prevent individuals from being able to develop optimal immune responses to Covid-19, and may thus inhibit the development of population immunity. If this was the case, we would expect to see the vaccinated become increasingly likely to be reinfected relative to the unvaccinated. In New Zealand and other countries around the world, we are indeed seeing the rates of covid infection becoming higher, on a per population basis, in the vaccinated than the unvaccinated.
What was I expecting from my test?
A paper (20) in the journal PNAS examined T-cell reactivity against COVID-19, and found that it was present for up to 20 months following infection in healthy individuals. The supplementary section of this paper contained some interesting raw data on both vaccinated and unvaccinated individuals. It included their levels of anti-S antibodies recorded at a range of days since infection up to nearly two years.
I took the raw data from the supplementary section and graphed the production of anti-S and anti-NC antibodies in vaccinated versus unvaccinated individuals across days since infection. You can see that vaccinated individuals (in red) have very high and persistent levels of anti-S antibodies compared to unvaccinated individuals (in blue). Consistent with the studies mentioned above, the unvaccinated produced significantly more anti-NC antibodies.


I used these results to roughly predict mine. Because my infection was about 140 days prior to my serology test, I expected to have very low or absent anti-S, but decent levels of anti-NC. This was in contrast to the Rako technician’s prediction of a 4 (positive) for anti-spike and negative nucleocapsid.
My results were in line with what I predicted: 1.8 (positive) for anti-NC, and 1 (equivocal) for anti-S.
A dear friend had her test the same day. She had no history of covid-19 infection (as far as she knew), and was double vaccinated. She was 0 (negative) for NC, and 7.3 (positive) for S. Although she had not been previously infected (as far as we know), her higher spike levels are consistent with the vaccinated group from the study above.
At this stage it is impossible to draw firm conclusions from my individual serology results, however it is interesting to see how they marry with some of the existing research, and to speculate as to what they might mean for my covid immunity. My guess is that I am probably protected from infection for some months (most of us will find that we catch covid on repeat, as we do colds and flus - some of us more often than others), and from severe disease on a long term basis. It is a shame that Rako is not collecting more data which would allow them to perform prospective studies which could confirm or disprove my guess. And it is a shame that the serology study being conducted in New Zealand excludes unvaccinated people.

Postscript
Since writing this, there has been a fascinating development involving the discovery that vaccination induces (in a dose-dependent manner) a rather dramatic conversion of antibodies to IgG4. IgG4 is the antibody formation responsible for tolerance: The Fc (crystallised fragment) of an IgG4 antibody tells your immune system “nothing to see here.” This is useful if you have a bee sting, or walk through a cloud of pollen - you don’t want your immune system to overreact to those. You do want your immune system to react to the spike protein in order to protect cells from damage. If the vaccine is inducing tolerance - does this mean we are setting up a situation in which mRNA vaccine-induced spike can travel unchallenged through the body, causing harm to tissues, and not being fought off and cleared? For now, we do not know the significance of this vaccine-induced conversion to spike tolerance, and can only speculate. I will write up this section more thoroughly soon.
* This study (Proteomics Clinical Applications, August 2023) found that although vaccine-induced spike antigen persisted for as long as six months, its levels did not correlate with antibodies.
References
Zoe Swank, Yasmeen Senussi, Zachary Manickas-Hill, Xu G Yu, Jonathan Z Li, Galit Alter, David R Walt, Persistent Circulating Severe Acute Respiratory Syndrome Coronavirus 2 Spike Is Associated With Post-acute Coronavirus Disease 2019 Sequelae, Clinical Infectious Diseases, 2022;, ciac722, https://doi.org/10.1093/cid/ciac722
Nabin K. Shrestha, Patrick C. Burke, Amy S. Nowacki, James F. Simon, Amanda Hagen, Steven M. Gordon. Effectiveness of the Coronavirus Disease 2019 (COVID-19) Bivalent Vaccine. medRxiv 2022.12.17.22283625; doi: https://doi.org/10.1101/2022.12.17.22283625
Paul R Hunter, Julii Brainard. Estimating the effectiveness of the Pfizer COVID-19 BNT162b2 vaccine after a single dose. A reanalysis of a study of ‘real-world’ vaccination outcomes from Israel. medRxiv 2021.02.01.21250957; doi: https://doi.org/10.1101/2021.02.01.21250957
Shrestha NK, Shrestha P, Burke PC, Nowacki AS, Terpeluk P, Gordon SM. Coronavirus Disease 2019 Vaccine Boosting in Previously Infected or Vaccinated Individuals. Clin Infect Dis. 2022 Dec 19;75(12):2169-2177. doi: 10.1093/cid/ciac327. PMID: 35476018; PMCID: PMC9129118.
Penn State. (2021, April 9). Antibody binding-site conserved across COVID-19 virus variants: The structural revelation could have implications as a therapeutic target in all SARS-CoV-2 variants. ScienceDaily. Retrieved December 6, 2022 from www.sciencedaily.com/releases/2021/04/210409124751.htm
Röltgen K, Nielsen SCA, Silva O, Younes SF, Zaslavsky M, Costales C, Yang F, Wirz OF, Solis D, Hoh RA, Wang A, Arunachalam PS, Colburg D, Zhao S, Haraguchi E, Lee AS, Shah MM, Manohar M, Chang I, Gao F, Mallajosyula V, Li C, Liu J, Shoura MJ, Sindher SB, Parsons E, Dashdorj NJ, Dashdorj ND, Monroe R, Serrano GE, Beach TG, Chinthrajah RS, Charville GW, Wilbur JL, Wohlstadter JN, Davis MM, Pulendran B, Troxell ML, Sigal GB, Natkunam Y, Pinsky BA, Nadeau KC, Boyd SD. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell. 2022 Mar 17;185(6):1025-1040.e14. doi: 10.1016/j.cell.2022.01.018. Epub 2022 Jan 25. PMID: 35148837; PMCID: PMC8786601.
Gazit S, Shlezinger R, Perez G, Lotan R, Peretz A, Ben-Tov A, Herzel E, Alapi H, Cohen D, Muhsen K, Chodick G, Patalon T. SARS-CoV-2 Naturally Acquired Immunity vs. Vaccine-induced Immunity, Reinfections versus Breakthrough Infections: a Retrospective Cohort Study. Clin Infect Dis. 2022 Apr 5:ciac262. doi: 10.1093/cid/ciac262. Epub ahead of print. PMID: 35380632; PMCID: PMC9047157
Wei J, Pouwels KB, Stoesser N, Matthews PC, Diamond I, Studley R, Rourke E, Cook D, Bell JI, Newton JN, Farrar J, Howarth A, Marsden BD, Hoosdally S, Jones EY, Stuart DI, Crook DW, Peto TEA, Walker AS, Eyre DW; COVID-19 Infection Survey team. Antibody responses and correlates of protection in the general population after two doses of the ChAdOx1 or BNT162b2 vaccines. Nat Med. 2022 May;28(5):1072-1082. doi: 10.1038/s41591-022-01721-6. Epub 2022 Feb 14. PMID: 35165453; PMCID: PMC9117148.
Lin DY, Gu Y, Xu Y, Zeng D, Wheeler B, Young H, Sunny SK, Moore Z. Effects of Vaccination and Previous Infection on Omicron Infections in Children. N Engl J Med. 2022 Sep 22;387(12):1141-1143. doi: 10.1056/NEJMc2209371. Epub 2022 Sep 7. PMID: 36069811; PMCID: PMC9511630.
Goldberg Y, Mandel M, Bar-On YM, Bodenheimer O, Freedman LS, Ash N, Alroy-Preis S, Huppert A, Milo R. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N Engl J Med. 2022 Jun 9;386(23):2201-2212. doi: 10.1056/NEJMoa2118946. Epub 2022 May 25. PMID: 35613036; PMCID: PMC9165562.
Busch MP, Stramer SL, Stone M, Yu EA, Grebe E, Notari E, Saa P, Ferg R, Manrique IM, Weil N, Fink RV, Levy ME, Green V, Cyrus S, Williamson PC, Haynes J, Groves J, Krysztof D, Custer B, Kleinman S, Biggerstaff BJ, Opsomer JD, Jones JM. Population-Weighted Seroprevalence From Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection, Vaccination, and Hybrid Immunity Among US Blood Donations From January to December 2021. Clin Infect Dis. 2022 Oct 3;75(Supplement_2):S254-S263. doi: 10.1093/cid/ciac470. PMID: 35684973; PMCID: PMC9214177.
A Tissue Distribution Study of a [3 H]-Labelled Lipid Nanoparticle-mRNA Formulation Containing ALC-0315 and ALC-0159 Following Intramuscular Administration in Wistar Han Rats, Test Facility Study No. 185350 Sponsor Reference No. ALC-NC-0552
Alana F Ogata, Chi-An Cheng, Michaël Desjardins, Yasmeen Senussi, Amy C Sherman, Megan Powell, Lewis Novack, Salena Von, Xiaofang Li, Lindsey R Baden, David R Walt, Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients, Clinical Infectious Diseases, Volume 74, Issue 4, 15 February 2022, Pages 715–718, https://doi.org/10.1093/cid/ciab465
Allen N, Brady M, Carrion Martin AI, Domegan L, Walsh C, Doherty L, Riain UN, Bergin C, Fleming C, Conlon N. Serological markers of SARS-CoV-2 infection; anti-nucleocapsid antibody positivity may not be the ideal marker of natural infection in vaccinated individuals. J Infect. 2021 Oct;83(4):e9-e10. doi: 10.1016/j.jinf.2021.08.012. Epub 2021 Aug 9. PMID: 34384812; PMCID: PMC8351117
UK Health Security Agency COVID-19 vaccine surveillance report Week 43
Heather J Whitaker, Charlotte Gower, Ashley D Otter, Ruth Simmons, Freja Kirsebom, Louise Letley, Catherine Quinot, Georgina Ireland, Ezra Linley, Sonia Ribeiro, Shamez Ladhani, Jamie Lopez-Bernal, Gayatri Amirthalingam, Mary E Ramsay, Kevin E Brown. Nucleocapsid antibody positivity as a marker of past SARS-CoV-2 infection in population serosurveillance studies: impact of variant, vaccination, and choice of assay cut-off. medRxiv 2021.10.25.21264964; doi: https://doi.org/10.1101/2021.10.25.21264964
Follmann D, Janes HE, Buhule OD, Zhou H, Girard B, Marks K, Kotloff K, Desjardins M, Corey L, Neuzil KM, Miller JM, El Sahly HM, Baden LR. Antinucleocapsid Antibodies After SARS-CoV-2 Infection in the Blinded Phase of the Randomized, Placebo-Controlled mRNA-1273 COVID-19 Vaccine Efficacy Clinical Trial. Ann Intern Med. 2022 Sep;175(9):1258-1265. doi: 10.7326/M22-1300. Epub 2022 Jul 5. PMID: 35785530; PMCID: PMC9258784
McGee C, Shi M, House J, Drude A, Gonzalez G, Martin N, Chen SH, Rogers H, Njunge A, Hodge X, Mosley B, George M, Agrawal R, Wild C, Smith C, Brown A, Barber L, Garantziotis S. Longitudinal Serological Surveillance for COVID-19 Antibodies after Infection and Vaccination. Microbiol Spectr. 2022 Oct 26;10(5):e0202622. doi: 10.1128/spectrum.02026-22. Epub 2022 Sep 19. PMID: 36121258; PMCID: PMC9603261
Movsisyan M, Chopikyan A, Kasparova I, Hakobjanyan G, Carrat F, Sukiasyan M, Rushanyan M, Chalabyan M, Shariff S, Kantawala B, Keshishyan A, Hovhannisyan A, Hakobyan A, Petrosyan G, Minasyan A, Muradyan A, Mekinian A, Yenkoyan K. Kinetics of anti-nucleocapsid IgG response in COVID-19 immunocompetent convalescent patients. Sci Rep. 2022 Jul 20;12(1):12403. doi: 10.1038/s41598-022-16402-0. PMID: 35859108; PMCID: PMC9297274
Martner A, Grauers Wiktorin H, Törnell A, Ringlander J, Arabpour M, Lindh M, Lagging M, Nilsson S, Hellstrand K. Transient and durable T cell reactivity after COVID-19. Proc Natl Acad Sci U S A. 2022 Jul 26;119(30):e2203659119. doi: 10.1073/pnas.2203659119. Epub 2022 Jul 12. PMID: 35858456; PMCID: PMC9335198
Lyngse, F.P., Mortensen, L.H., Denwood, M.J. et al. Household transmission of the SARS-CoV-2 Omicron variant in Denmark. Nat Commun 13, 5573 (2022). https://doi.org/10.1038/s41467-022-33328-3